UnderBite Treatment!!!
9월 30, 2022
Should I have double jaw surgery, which is currently being done worldwide?
9월 30, 2022Neuromuscular physiological position/MCB splint position.
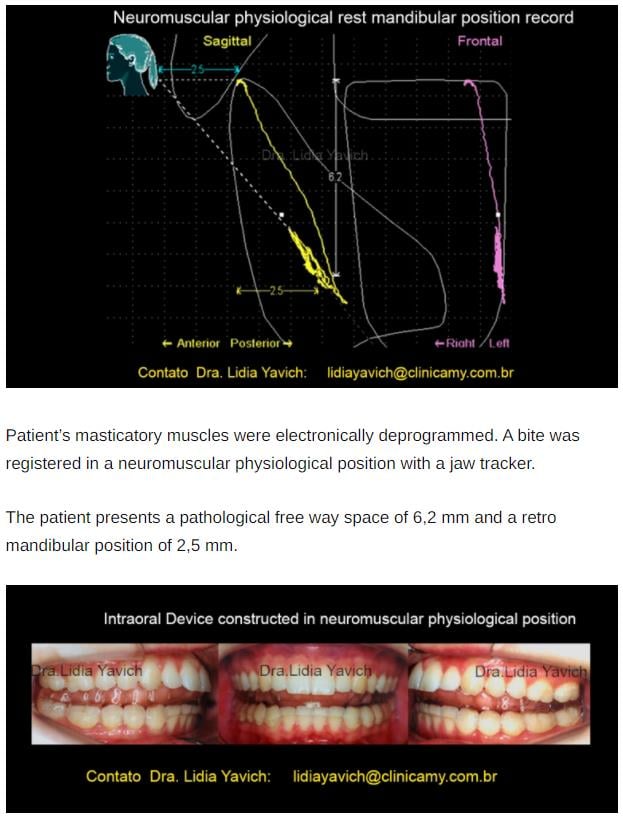
A bite was registered in a neuromuscular physiological position with a jaw tracker.
The patient presents a pathological free way space of 6,2 mm and a retro mandibular position of 2,5 mm.
In the jaw tracker, the neuromuscular pathological free way space can be as high as 10 mm. I think this is similar to the height when the occipital bone moves normally in the MCB splint. If this 10mm height changes to an ideal 1mm free way space, a change of 9mm is required. Such a large amount of change cannot be obtained only with the teeth, and must be obtained through positional changes in the maxilla, temporal bone and mandible to finally achieve an occlusion with an ideal 1mm free way space.(MCB/H)
The left and right position of the splint is slightly different from the neuromuscular physiological position. In the MCB splint, it is set at a position where the sphenoid bone moves well, not at the left and right position at the jaw joint.
These treatments require the teeth to occlude in this position, unless the position of the skull bone changes.
However, in MCB splint treatment, the initially set height differs depending on the individual, and these position change the position of the temporal bone, mandible and discs as the movement of the skull improves, and the height gradually decreases as the number of MCB splint treatments increases. At the end of the treatment, the skull is in a position to improve movement, and the teeth will occlude at a lower height rather than the higher height initially set.
I do orthodontic treatment so that the teeth are occluded at a height that does not change anymore in the MCB/L and the height remains constant. I can check the 3D position of the lower jaw at any time during treatment, without the help of a jaw tracker.
I understand that Dr. Brendan Stack's treatment method was treated similarly to the above.